EDITORIAL
PHOTOGRAPHY
WRITING
VIDEO
PAGE DESIGN
PODCAST
EDITOR-IN-CHIEF
COMMERCIAL
MUSIC
PORTRAITS
ABOUT
CONTACT
EDITORIAL
PHOTOGRAPHY
WRITING
VIDEO
PAGE DESIGN
PODCAST
EDITOR-IN-CHIEF
COMMERCIAL
MUSIC
PORTRAITS
ABOUT
CONTACT
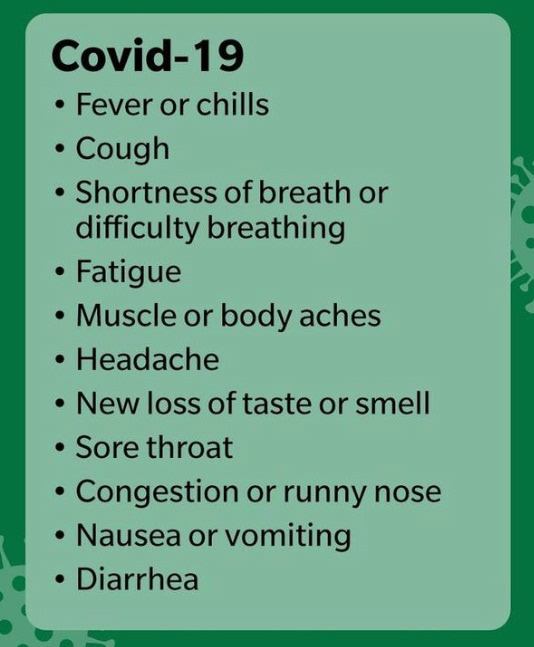
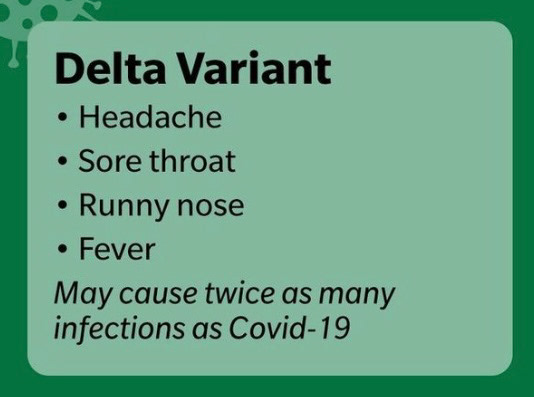
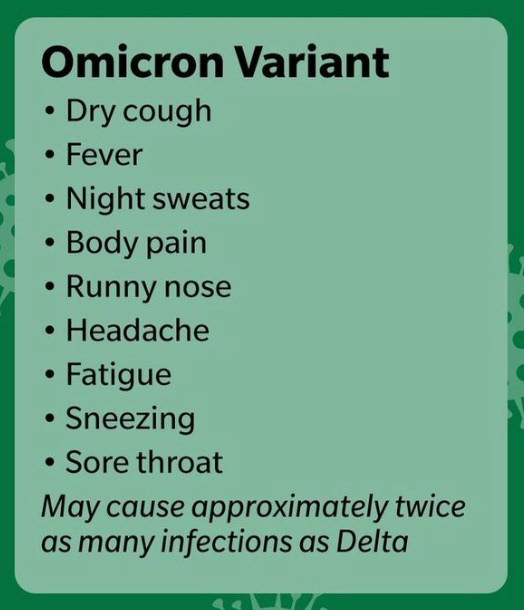
COVID ACKNOWLEDGEMENT FORM
Responses to this form remain confidential. Form response required for the safety of you, others around you, and photographers/assistants.
Name *
Phone Number *
Shoot Date *
Do you have cold or flu like symptoms, such as fever, chills, muscle pain, or sore throat? *
Do you have a NEW onset of cough or shortness of breath? *
Have you had close contact with someone who has been diagnosed with COVID-19 within the past 14 days? *
Do you have a NEW onset of loss of taste and/or smell? *
Has it been less than 10 days since your symptoms began? *
Please acknowledge that if you have answered yes to any of these questions, you MUST call/text or email ASAP. No fee will be charged for a reschedule if necessary. *
ANY SYMPTOMS NOT LISTED IN THE QUESTIONS ABOVE? *
Submit
Thank you!
↑
Back to Top